SHOULD THE FDA RUSH PFIZER’S COVID VACCINE EUA FOR KIDS?
Updated






By Jefferey Jaxen
Today is the last day for public comment on the U.S. Food and Administration’s (FDA) upcoming Vaccines and Related Biological Products Advisory Committee meeting scheduled for October 26th. On the docket will be discussion on recommending an Emergency Use Authorization for Pfizer BioNTech mRNA COVID 19 vaccine for children 5-11 years of age. Let’s look at some of the data we know to date.
In early October of 2021, Reuters reported that both Sweden and Denmark were pausing the use of Moderna’s mRNA COVID-19 vaccine for younger age groups after reports of possible rare cardiovascular side effects. Finland joined days later with an identical suspension of the shot for the same reasons. Similarly, the non-EU Norwegian Institute of Public Health urged young people under 30 to opt for the Pfizer vaccine “due to an increased risk of a rare side effect” with Moderna.
There have been continued, well-documented risks of myocarditis in younger adults receiving mRNA vaccines. Israel, who led the world in the early vaccination of their younger age groups with the Pfizer BioNTech mRNA COVID 19 vaccine, produced data recently foreshadowing the great myocarditis risk game being played around the world.
Two studies published in the New England Journal of Medicine (NEJM) showed an increased risk of myocarditis in younger age groups. One showing patients in Israel’s largest healthcare system, Clalit Health Services, estimated an incidence of myocarditis of 2.13 cases per 100,000 vaccinated persons, reaching as high as 10.69 cases per 100,000 in men and boys ages 16 to 29.
The other, as reported in medpagetoday.com, used Israel’s government database and captured active and passive periods of surveillance for myocarditis. This study supported the higher risk in young men finding males of all ages had myocarditis occur at 0.64 cases per 100,000 persons after the first dose and 3.83 cases per 100,000 after the second dose — with the incidence increasing to 1.34 and 15.07 per 100,000 after the first and second doses, respectively, for teenage boys ages 16 to 19.
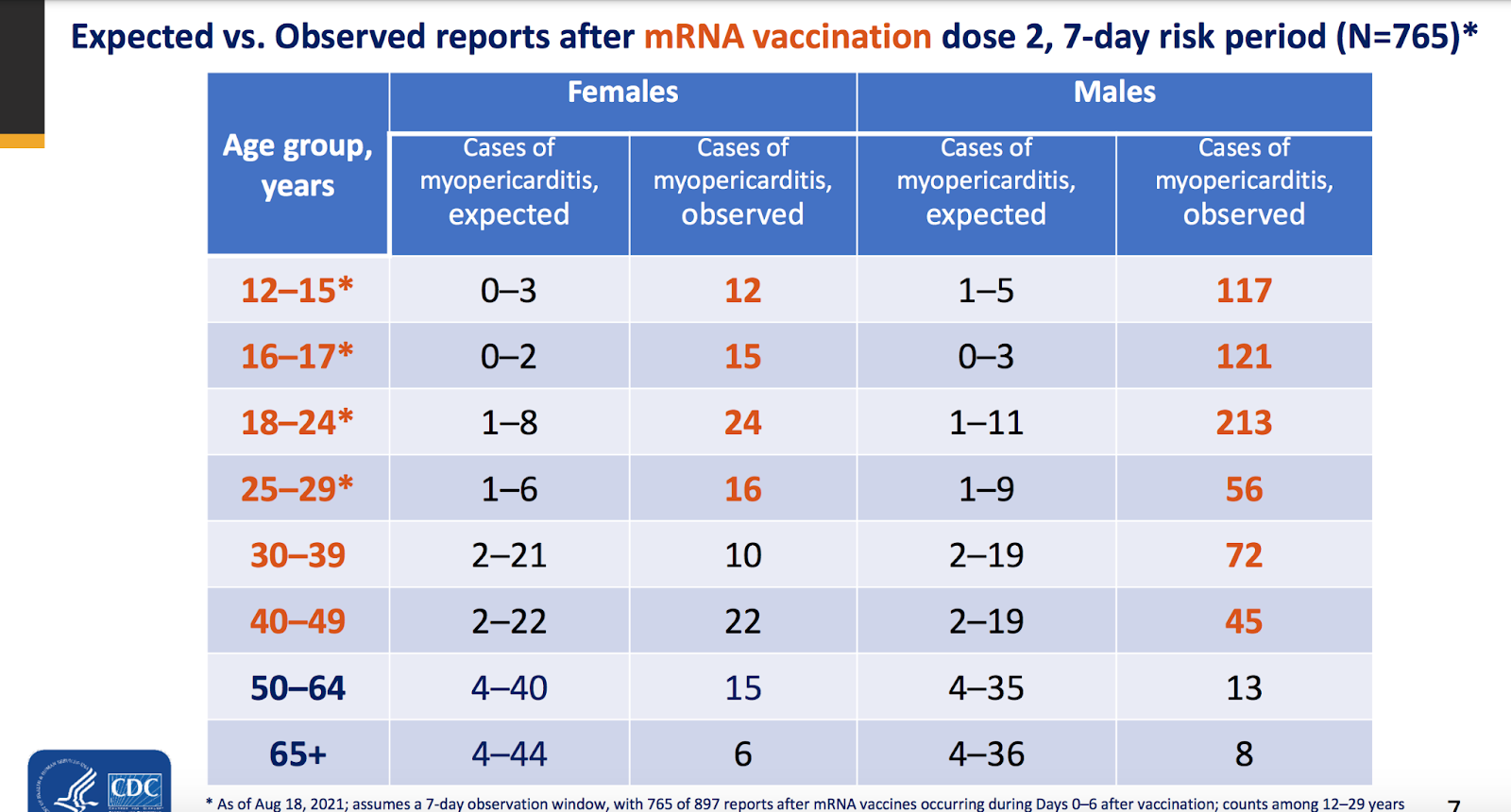
Even the Center For Disease Control and Prevention’s (CDC) own Advisory Committee on Immunization Practices (ACIP) data found a substantial increase in myocarditis in young adults. A presentation by a CDC COVID-19 Vaccine Task Force member in April showed data on expected (background) rates of myocarditis and pericarditis compared to what was being captured in the (passive) vaccine adverse events reporting system (VAERS). The slide below tells the story:
Despite the pleas by public health officials that myocarditis is a mild, self-correcting condition, literature has shown that the sudden onset of heart inflammation may be more than a background medical event. A review article published in 2019 stated State of the art: Evaluation and prognostication of myocarditis using cardiac MRI stated, “Acute, nonfulminant myocarditis, conversely, has a more indolent presentation with increased mortality up to 20% in the first year and 55% at 11 years based on initial diagnosis of acute myocarditis.”
The review continues to state, “Up to 12% of sudden cardiac deaths are attributed to myocarditis, with arrhythmia as the most common mechanism.”
Another argument purportedly supporting the need to rush an EUA for children, that the predominant Delta variant is more deadly in children, was proven false by a recent study looking at UK school-aged children. The study looked at the illness profile of SARS-CoV-2 (symptom prevalence, duration, and burden), hospital presentation, and presence of long (≥28 day) illness in 694 children (276 younger [5-11 years]) symptomatic children tested positive for SARS-CoV-2 with Alpha infection and 706 (227 younger and 479 older) children with Delta infection.
Their findings led them to conclude that the Delta variant resembles illness due to the Alpha variant “with short duration and similar symptom burden.”
With the elevated risk profiles presenting as safety signals for both myocarditis and pericarditis being seen in younger adults, there is no reason to expect such risks wouldn’t carry into the younger 5-11 year old age group. Despite the media hype around protecting kids from COVID-19, there appears to be no clear and present pandemic-level danger. The American Academy of Pediatrics (AAP), responsible for state-level collecting and reporting on publicly available data from states on child COVID-19 cases, showed the following data in its latest update.
Since AAP’s reporting start date of April of 2020, cumulative hospitalizations (24 states and NYC reported) of children ranged from 1.6%-4.3% of their total cumulated hospitalizations and 0.1%-2.0% of all their child COVID-19 cases resulted in hospitalization
Child mortality figures from 45 states (NYC, PR and GU reported) showed children were 0.00%-0.26% of all COVID-19 deaths, and 7 states reported zero child deaths. In states reporting, 0.00%-0.03% of all child COVID-19 cases resulted in death.
In a July 2021 WSJ opinion piece titled The Flimsy Evidence Behind the CDC’s Push to Vaccinate Children, Marty Makary M.D., M.P.H. writes, “A tremendous number of government and private policies affecting kids are based on one number: 335. That is how many children under 18 have died with a Covid diagnosis code in their record, according to the Centers for Disease Control and Prevention. Yet the CDC, which has 21,000 employees, hasn’t researched each death to find out whether Covid caused it or if it involved a pre-existing medical condition.”
Makary concludes, “My research team at Johns Hopkins worked with the nonprofit FAIR Health to analyze approximately 48,000 children under 18 diagnosed with Covid in health-insurance data from April to August 2020. Our report found a mortality rate of zero among children without a pre-existing medical condition such as leukemia.”
Another aspect of scientific data unrecognized by public health authorities, such as the CDC, is the protection offered by natural immunity. Attorneys for the Informed Consent Action Network (ICAN) recently provided the CDC with over 60 studies reflecting that natural immunity is more durable and robust than vaccine immunity. The volume of studies is flying in the face of a media narrative which claims children are a reservoir for the COVID-19 virus. The inflammatory statements were backed up by the limited research of just one study of 110 Covid-19 patients aged two weeks to 21 years in which the researchers did not find a correlation between viral load and severity of the disease in kids.
Are cases of COVID are increasing in kids? Have they become contagious, asymptotic carries? More studies have shed light on those questions as well. A May 2021 study at the fifth-largest children’s hospital in the country looked at 146 records listing patients as positive for SARS-CoV-2 from May 1, 2020, to September 30, 2020, the authors classified 58 (40 percent) as having “incidental” diagnosis, meaning there was no documentation of COVID-19 symptoms prior to hospitalization.
The study categorized 68 patients, or 47 percent, as “potentially symptomatic,” which was defined as when “COVID-19 was not the primary reason for admission for these patients, and COVID-19 alone did not directly require hospitalization without the concomitant condition.”
With several unanswered questions about SARS-CoV-2 infection in younger children, the already known increase in heart inflammation risks associated with Pfizer’s shot and the growing body of evidence showing the superiority of natural immunity, what choice will the FDA make tomorrow on the EUA vote?
To register a comment with the FDA before their vote, visit this link TODAY